Pain related evoked potentials in spinal cord pathology
Project Leader PD Dr. Martin Schubert
In chronic spinal cord disorders, such as degenerative cervical myelopathy (DCM), spinal tumors, ischemia or syringomyelia, clinical symptoms may initially be minor and these pathologies are thus prone to be missed due to gradual onset. As this is a potential cause for delayed diagnosis and treatment of such conditions, it is crucial to develop sensitive neurophysiological diagnostic tests to provide for objective benchmarks for their early detection. While standard neurophysiological tests such as somatosensory evoked potentials (SSEPs) are not sensitive enough to detect impaired spinal conduction in these pathologies, noxious stimuli such as contact heat evoked potentials (CHEPs) allow for specific testing of spinothalamic propagation and demonstrate superior sensitivity for detecting impaired spinal conduction due to their special neuroanatomy with segmentally crossing spinothalamic fibers. However, contact heat stimulation is technically challenging and requires equipment that is not available to standard neurophysiological laboratories. Therefore, intra-epidermal electrical stimulation (IES), another type of noxious stimulation, has been proposed as a more accessible option for nociceptive testing in clinical routine.
In this project we compare IES to contact heat stimulation as an alternative noxious stimulus. Intra-epidermal electrically evoked potentials (IEEPs) similar to CHEPs so far showed good clinical applicability and a high sensitivity to detect cervical myelopathy in 27 patients with DCM compared to healthy controls. Results suggest that IES effectively activates the spinal pain pathway, thereby providing a diagnostic alternative to heat pain stimulation. In order to further validate this diagnostic method, it has to be tested in other spinal pathologies with sensory deficits pertaining to nociception (spinal syndromes: Brown Séquard, Anterior Cord).
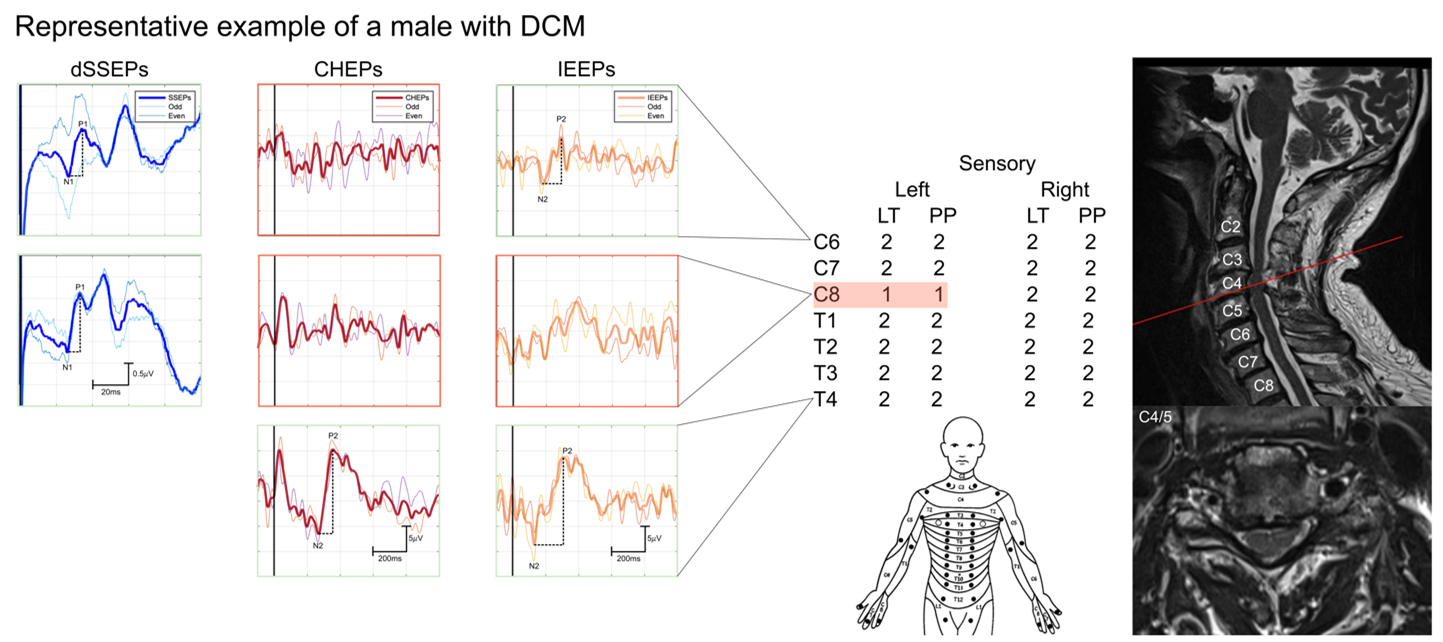
Representative example of clinical bedside testing and neurophysiological findings in a 64-year-old male with DCM at C4/5 level.
Cervical and thoracic sensory scores (0 & 1 = impaired, 2 = normal) from clinical examination. Red shading highlights the sensory loss at segmental level C8 with lower light touch (LT) and pinprick and (PP) scores on the left side. Normal dSSEPs indicate lack of sensitivity for detection while a segmental loss of CHEPs as well as of IEEPs for stimulation of left C6 and C8 dermatomes allow objective detection of a deficit. Color frames indicate categories for the evaluation of each evoked potential, i.e., red: absent, pink: abnormal, and blue: normal. Sagittal cervical (C2-C8) and axial slices (C4/5) of T2-weighted magnetic resonance imaging scans of the level of maximum stenosis are shown on the right. Note that there were neither MR signs of myelopathy nor radicular compression (Júlio et al., Clin.Neurophys. 2024)
.